Today we’re sharing part pour of our series with Dr. Neil Feldman. In the final installment, we take a deep dive into other elements to consider for a proper shoe fit and why they are important.

The last of the three main categories is shoe fit and I’ll make an analogy here:
A Toyota Corolla is never going to beat a Ferrari in a road race. A Ferrari is never going to survive an off-road race against a Jeep.
These cars are built differently and thus serve different purposes. What is most important to the function, and ultimate survivability of these cars’ performance, is having the right tires (feet) underneath them. Equally as important, is having proper car alignment (posture) so that the load is distributed appropriately. If the car has bad alignment, and is driven in a way that is beyond the cars’ ability, then the wheels have no chance of holding up. If you have bad posture, then your feet have little chance of holding up when they are being asked to work in a way that goes beyond the body’s ability. Thus is the interdependent nature of foot problems and body problems and how to solve them.
Bunions, arthritic big toe joints, ball of foot/sesamoid problems and neuroma’s (thickened nerve usually between the 3rd and 4th toes that can cause burning and numbness in the ball of the foot and those toes) would almost be non-existent if not for the negative impact of forcing your foot into a space that prevents it from developing naturally without being restricted.
Our feet have 28 bones and 20 distinct muscles that originate in the foot (intrinsic muscles of the foot). I like to think of these muscles as stabilizers for our feet. Our lower legs have another 11 muscles that attach somewhere in the foot and serve as the “movers” of the foot (extrinsic muscles). I use quotations because the function of the muscles will depend on if the foot is on or off the ground when they fire, as well as at which moment during gait cycle they are active in. The key point to understand is that we have a group of muscles that are large and help move the foot (extrinsic) and another group of muscles (intrinsic) that are small and help stabilize the foot WHEN being moved.
The best way to strengthen anything in our bodies is to use that part of our body.
Being barefoot and wearing shoes that are soft is one of the easiest and best way to strengthen those small, intrinsic muscles. Conversely, binding your foot in a shoe too small and wearing stiff shoes from an early age is one of the best ways to prevent proper development of the stabilizing intrinsic foot muscles.
The result of having the movers of the foot be strong and the stabilizers of the foot be weak is bunions, hammertoes, arch pain, midfoot arthritis, etc. The metatarsals not being allowed to spread as they should is the best way to develop a neuroma, just as with a tapered toe box that doesn’t allow the big toe to spread like it should with the metatarsal is the best way to develop a bunion. Finding the best possible shoe fit will be the best solution to any of these problems.
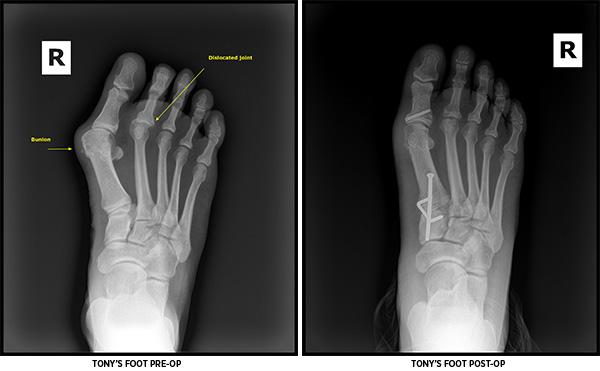
And finally, full circle back to Tony:
Tony’s problems were the end result of years of adapted movement and poor-fitting shoes for his feet. The solution for him was a challenge given how long the dislocation existed and the fixed structural changes to the joints in question. In order to stabilize his foot, the middle part of his foot that was arthritic and unstable needed to be stabilized. We fused it in a better position to provide needed First ray stability (locking that unstable part of the tripod) and improved big-toe joint alignment, hopefully allowing the repair of the 2nd toe dislocation to last a lifetime. Because Tony’s 2nd toe had been dislocated for so many years, there was very little that could be done to put the toe back in place and hold it there.
A common approach is to shorten the metatarsal to reduce the loading forces through the joint and then repair the ligaments that are supposed to stabilize the toe at the level of the joint. He had no ligaments left to repair. Tony also did not have a healthy metatarsal head: the toe damaged the cartilage when it dislocated and then all of his weight was placed through the damaged metatarsal. So essentially Tony endured decades of strain via ongoing physical activity without a functional big toe joint!
In order to straighten his 2nd toe, repair the dislocation and maintain stability through the front of his foot, Tony also underwent a procedure where part of his metatarsal was removed and shortened; the toe was fused straight and the dislocation repaired with temporary pinning and a stable, improved alignment that will be held together with the scarring of the tissues under the newly positioned joint. Tony was off of his feet for almost 2 months and has another 2 months of slowly getting back to everyday life and activity. He’s using a foot that has been surgically reshaped and made functionally more stable, albeit not as it was meant to be.

About Dr. Feldman
Dr. Neil Feldman is the Director of Central Massachusetts Podiatry., specializing in reconstructive surgery and sports medicine. With more than 20 years of private practice experience, Dr. Feldman is board-certified in Foot Surgery, active in the Massachusetts Podiatric Medical Society and is a Fellow of the American College of Foot and Ankle Surgeons. Previously, he served on the Massachusetts Podiatric Medical Association Board.
An accomplished athlete, Dr. Feldman has run numerous marathons, including 12 Boston Marathons, and clocked in a personal best of 2:51 at the Bay State marathon in 2013. He also completed 7 Ironman triathlons, including the Ironman World Championships Kona in 2004 and 2008. He also took his endurance running endeavors to new lengths when he completed seven 100M events, including 2 Leadville finishes and twice breaking 20 hours at that distance while sporting the MT-3 (Javelina Jundred in 2016) and Terraventure (Vermont 100M in 2017).